
TL;DR:
- Untreated fungal toenails can spread and cause pain, infections, and mobility issues. Accurate diagnosis and a combination of treatments are essential for effective eradication. Preventive habits are crucial to reduce the risk of recurrence over time.
Onychomycosis, the medical term for fungal toenail infection, is defined as a chronic fungal invasion of the nail plate, bed, or matrix. It is not a cosmetic nuisance you can safely ignore. Onychomycosis accounts for about 50% of all nail disorders and can lead to pain, walking difficulty, and secondary bacterial infections if left untreated. Understanding why treat fungal toenails matters is the first step toward protecting your foot health and avoiding complications that go well beyond a discolored nail.
Why treat fungal toenails before they get worse
Treating fungal toenails stops a progressive infection before it causes lasting damage to the nail structure, surrounding skin, and your ability to walk comfortably. Left alone, the infection does not stabilize. It spreads. The nail thickens, becomes brittle, and separates from the nail bed, a process called onycholysis. Pain follows, and so do more serious complications.
Nail fungus is a chronic infection that rarely clears without medical intervention and often spreads if ignored. That finding matters because most patients delay care by months or years, assuming the nail will improve on its own. It almost never does.
The consequences of untreated fungal nails include:
- Thickened, distorted nails that press against footwear and cause direct pain
- Spread to adjacent nails and surrounding skin, including tinea pedis (athlete’s foot)
- Secondary bacterial infections, particularly dangerous for patients with diabetes or poor circulation
- Gait changes caused by nail pain, which can stress the knees, hips, and lower back over time
- Reduced quality of life, including avoidance of social situations, swimming, or physical activity
Patients with diabetes or peripheral vascular disease face elevated risk of complications from untreated fungal nails and should seek prompt professional evaluation. For these patients, a thickened nail can become a gateway to ulceration or serious soft tissue infection.
Fungal toenails are not a waiting game. The infection does not plateau. Without treatment, the fungus colonizes deeper nail structures, spreads to neighboring nails, and creates conditions that invite bacterial co-infection. The longer you wait, the harder the infection is to eradicate.
The connection between foot health and mobility is direct. When nail pain changes how you walk, the effects ripple upward through your entire musculoskeletal system.
How are fungal toenails diagnosed, and why does it matter?
Accurate diagnosis is the foundation of effective treatment. A clinical exam alone is not enough. Several nail conditions mimic onychomycosis closely, and treating the wrong condition wastes time, exposes you to unnecessary medication, and allows the real problem to progress.
Conditions that look like fungal nails include:
- Nail psoriasis, which causes pitting, oil-drop discoloration, and subungual hyperkeratosis
- Traumatic nail dystrophy from repetitive pressure or injury
- Lichen planus, a less common inflammatory condition affecting the nail matrix
- Green nail syndrome, caused by bacterial rather than fungal infection
Confirming diagnosis with lab tests before treatment is critical to avoid misdiagnosis and unnecessary drug exposure. The standard diagnostic tools are microscopy (KOH preparation), fungal culture, and PCR testing. PCR is the fastest and most sensitive method, but culture remains the gold standard for identifying the specific organism.
Why does organism identification matter? Different fungi respond to different antifungals. Dermatophytes like Trichophyton rubrum respond well to terbinafine. Non-dermatophyte molds and Candida species may require different agents entirely. Treating without knowing the organism risks treatment failure from the start.
Pro Tip: Ask your podiatrist to send nail clippings for both microscopy and culture before starting any oral antifungal. This two-step confirmation reduces the chance of treating a non-fungal condition and guides the most effective drug choice.
Nail matrix involvement predicts more severe infections that are harder to eradicate and require systemic therapy. A podiatric evaluation identifies matrix involvement early, which directly shapes the treatment plan. Skipping professional evaluation and self-treating with over-the-counter products almost always results in incomplete treatment of a more serious infection.
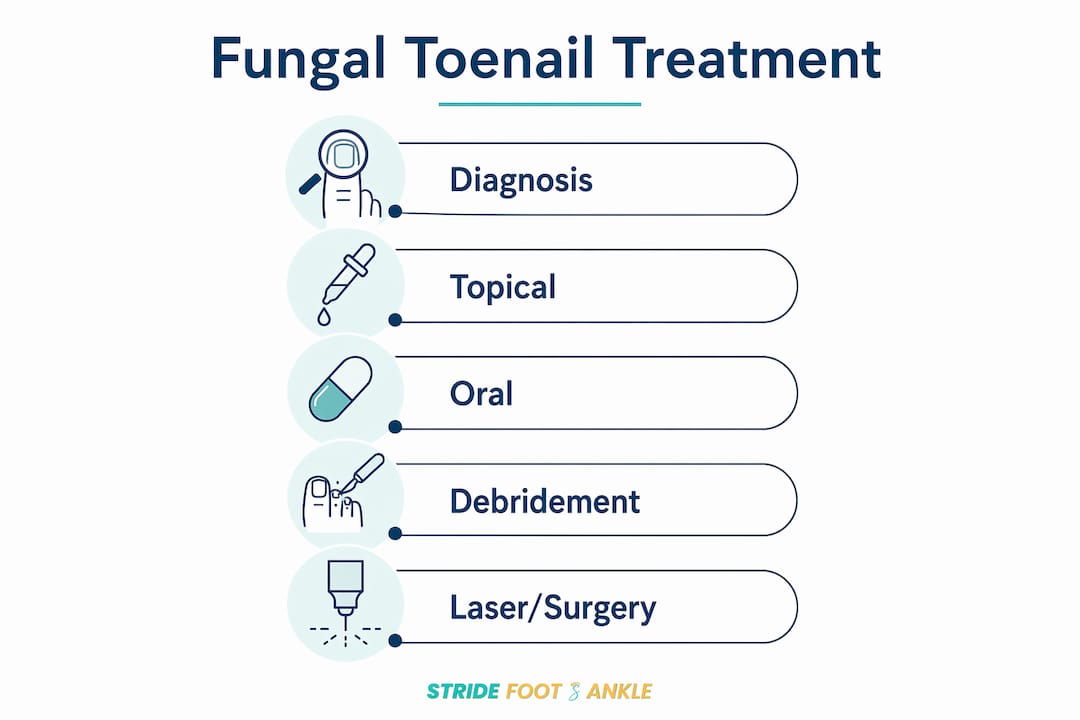
What are the effective treatment options for fungal toenails?
Effective treatment for onychomycosis combines the right medication, mechanical nail care, and lifestyle adjustments. No single approach works for every patient. The choice depends on the organism identified, the severity of nail involvement, and your overall health.
Topical antifungals
Topical agents work best for mild to moderate infections that have not reached the nail matrix. Approved topical options include ciclopirox nail lacquer, efinaconazole solution, tavaborole solution, and amorolfine nail lacquer. These agents penetrate the nail plate to reach the nail bed, but their cure rates are lower than oral therapy. They are most effective when used alongside mechanical debridement.
Oral antifungals
Oral therapy is the most effective treatment for moderate to severe onychomycosis. Oral terbinafine requires a 12-week course and achieves mycological cure in 70–80% of patients, making it the gold standard for fungal nail treatment. That cure rate is meaningful: it means most patients who complete the full course clear the infection at the fungal level, even before the nail fully grows out.
Itraconazole and fluconazole are alternatives for patients who cannot tolerate terbinafine or who have non-dermatophyte infections. Itraconazole is often prescribed as pulse therapy, one week on and three weeks off, repeated over several months. Fluconazole is used weekly for extended periods. Both are effective but carry their own drug interaction profiles that require medical review.
Mechanical debridement
Mechanical nail debridement is essential to enhance topical and systemic treatment by reducing nail thickness and improving drug penetration. A podiatrist uses specialized instruments to thin and trim the infected nail, removing the bulk of fungal material and allowing medication to reach deeper layers. Patients who skip debridement consistently show slower and less complete responses to treatment.
Laser therapy and surgical options
Laser therapy shows promise as an adjunct treatment but is not currently first-line due to limited evidence and recurrence rates. Major podiatric guidelines do not recommend laser as a standalone therapy. It may be useful for patients who cannot take oral medications or as a complement to topical treatment.
Surgical nail removal is reserved for cases where the nail is severely damaged, causing persistent pain, or where infection has not responded to other approaches. Partial or complete nail avulsion removes the infected tissue and allows a fresh nail to grow in its place.
Pro Tip: Combination therapy using oral and topical agents plus mechanical debridement maximizes cure rates. If your treatment plan includes only one of these elements, ask your podiatrist whether adding the others makes sense for your case.
| Treatment type | Best use case | Typical duration | Approximate cure rate |
|---|---|---|---|
| Oral terbinafine | Moderate to severe dermatophyte infection | 12 weeks | 70–80% mycological cure |
| Oral itraconazole | Non-dermatophyte or terbinafine intolerance | Pulse therapy, 3–4 months | Comparable to terbinafine |
| Topical efinaconazole | Mild infection, no matrix involvement | 48 weeks | Lower than oral |
| Mechanical debridement | Adjunct to all therapies | Ongoing as needed | Enhances other treatments |
| Laser therapy | Adjunct, oral medication contraindicated | Variable | Limited standalone evidence |
One reality patients often underestimate: even after mycological cure, the nail takes 12–18 months to grow out fully and appear normal. Treatment success is not visible immediately. Successful treatment requires patient education about the chronic nature of the infection and the long timeline for healthy nail growth. Stopping medication early because the nail “looks better” is one of the most common reasons treatment fails.
How can you prevent fungal toenail infection and recurrence?
Prevention is not optional after treatment. Recurrence affects up to 50% of patients within five years due to environmental reservoirs and host factors. That statistic means clearing the infection once is only half the work. Without consistent preventive habits, reinfection is likely.
Follow these steps to protect your nails after treatment:
- Keep feet clean and dry. Wash feet daily with soap and water. Dry thoroughly between the toes, where moisture lingers longest and fungal growth is most likely.
- Change socks daily. Wear moisture-wicking socks made from synthetic fibers or wool rather than cotton, which retains moisture. Change socks immediately after exercise.
- Wear breathable footwear. Shoes made from leather or mesh allow airflow and reduce the warm, humid environment that fungi thrive in. Rotate shoes to allow them to dry between wearings.
- Treat athlete’s foot promptly. Treating underlying athlete’s foot and maintaining footwear hygiene are necessary to prevent fungal recurrence after treatment. Tinea pedis on the skin is the most common source of nail reinfection.
- Disinfect or replace contaminated footwear. Antifungal sprays or powders applied inside shoes kill residual spores. Heavily contaminated shoes that cannot be disinfected should be replaced.
- Avoid sharing nail care tools. Nail clippers, files, and scissors can transfer fungal spores between people. Use your own tools and sterilize them with isopropyl alcohol after each use.
- Use caution at nail salons. Confirm that your salon sterilizes instruments between clients. Pedicure tools that are not properly sterilized are a well-documented transmission route.
- Monitor regularly if you are at risk. Patients with diabetes, peripheral vascular disease, or immunosuppression need ongoing monitoring. Patients with comorbidities such as diabetes or immunosuppression need individualized treatment and close follow-up to avoid complications.
Pro Tip: Apply an antifungal powder or spray to the inside of your shoes every morning, especially if you wear closed-toe shoes for long periods. This single habit significantly reduces the fungal load in your footwear environment.
Preventing reinfection also means addressing the foot fungus risk factors that made you vulnerable in the first place. Sweaty feet, tight shoes, and communal environments like gym locker rooms all raise your baseline risk. Changing those habits is as important as any medication.
Key takeaways
Treating fungal toenails is a medical necessity, not a cosmetic choice, because untreated onychomycosis spreads, causes pain, and creates serious complications for at-risk patients.
| Point | Details |
|---|---|
| Treat early, not late | Fungal nails rarely self-resolve and worsen significantly without medical intervention. |
| Confirm diagnosis first | Lab testing before treatment prevents misdiagnosis and guides the correct antifungal choice. |
| Oral terbinafine leads | A 12-week course achieves 70–80% mycological cure, the highest rate of any single agent. |
| Debridement improves outcomes | Thinning the nail mechanically allows medication to penetrate deeper and work more effectively. |
| Recurrence is common | Up to 50% of patients see recurrence within five years without consistent preventive habits. |
What I’ve learned treating fungal nails over the years
The most consistent pattern I see is delay. Patients arrive after months or years of watching a nail change color and thicken, convinced it was “just cosmetic.” By the time they come in, the infection has often spread to two or three nails, and the nail matrix is involved. That changes the treatment entirely.
The second pattern is unrealistic expectations about timeline. Patients start oral terbinafine, feel no visible change after six weeks, and stop. They interpret the absence of immediate visual improvement as treatment failure. The nail looks the same because the infected portion is still growing out. The medication is working at the root. Stopping early is the single most common reason I see treatment fail and recurrence follow.
What actually works is a combination approach: confirm the organism, start oral therapy, debride the nail regularly, and address the skin simultaneously. Treating the nail without treating concurrent athlete’s foot is like fixing a leak while leaving the water running. The infection returns from the skin within months.
I also want to be direct about laser therapy. Patients ask about it frequently because it sounds modern and painless. The evidence does not support it as a standalone treatment. It may have a role as an adjunct, but patients who choose laser over oral medication because they want to avoid systemic drugs are accepting a significantly lower chance of cure.
The most encouraging thing I can tell you is that onychomycosis is treatable. With the right diagnosis, the right medication, and consistent follow-through, most patients achieve clear nails. The key is starting, staying the course, and not letting the slow timeline discourage you.
— Ramil
Fungal toenail care at Stridefootankle
Stridefootankle provides comprehensive foot and ankle care for patients dealing with fungal toenails, from accurate diagnosis through treatment and long-term prevention. Dr. Nahad Wassel combines clinical nail evaluation, laboratory confirmation, mechanical debridement, and prescription antifungal therapy into individualized care plans designed for each patient’s specific infection and health profile.

Whether you are noticing early nail discoloration or dealing with a longstanding infection across multiple nails, a professional evaluation at Stridefootankle gives you a clear picture of what you are dealing with and a realistic path to healthier nails. Patients in Las Vegas can request an appointment directly through the Stridefootankle website and get started with a plan that addresses both the infection and the factors that put you at risk for recurrence.
FAQ
What are the main symptoms of fungal toenails?
Fungal toenails typically appear yellow, brown, or white, and become thickened, brittle, and crumbly over time. The nail may separate from the nail bed and emit an unpleasant odor as the infection progresses.
Can fungal toenails go away without treatment?
Fungal toenails rarely resolve without medical treatment. The infection is chronic by nature and almost always worsens or spreads to other nails and surrounding skin without intervention.
How long does treatment for fungal toenails take?
Oral terbinafine requires a 12-week course, but the nail takes 12–18 months to grow out fully and appear normal. Patients should expect a long timeline and complete the full medication course even when improvement is not yet visible.
Are fungal toenails dangerous for people with diabetes?
Patients with diabetes or peripheral vascular disease face significantly higher risks from untreated fungal nails, including secondary bacterial infections and potential ulceration. Prompt professional evaluation is strongly recommended for this group.
How do you prevent fungal toenails from coming back?
Preventing recurrence requires treating concurrent athlete’s foot, keeping feet dry, wearing breathable footwear, disinfecting shoes regularly, and avoiding shared nail tools. Up to 50% of patients experience recurrence within five years without consistent preventive habits.
Recommended
- Fungal Toenails: Treatments, Remedies, and Prevention – Stride Foot & Ankle – Dr. Nahad Wassel
- What Is Nail Fungus? Causes, Symptoms, and Treatment – Stride Foot & Ankle – Dr. Nahad Wassel
- Understanding Foot Fungus and When to Seek Help – Stride Foot & Ankle – Dr. Nahad Wassel
- Ingrowing Toenails: Causes, Relief, and Treatment – Stride Foot & Ankle – Dr. Nahad Wassel
Recent Comments