
TL;DR:
- Bracing uses supportive devices to stabilize and promote healing in injured ankles and feet. Selecting the appropriate brace, such as lace-up, stirrup, walking boot, or custom orthosis, depends on injury severity and individual needs. Proper use, consistent wear, and combining bracing with physical therapy enhance recovery and reduce reinjury risk.
Bracing is the use of supportive or immobilizing devices, such as ankle braces, walking boots, and custom ankle-foot orthoses (AFOs), to protect injured foot and ankle structures and promote recovery. The right brace stabilizes damaged ligaments, tendons, or bones while allowing the controlled movement your body needs to heal. Choosing the wrong device, or skipping professional guidance entirely, can slow recovery or worsen the injury. This guide explains every major bracing option, how each one works, and how to match the right device to your specific condition.
What are the main types of foot and ankle braces?
Foot and ankle bracing falls into four broad categories, each designed for a different level of injury severity and functional need. Ankle braces stabilize through compression and mechanical restriction for mild-to-moderate sprains, while walking boots provide rigid immobilization for severe injuries and post-surgery recovery. Knowing which category fits your diagnosis is the first step toward effective treatment.

Lace-up ankle braces
Lace-up braces are the most common over-the-counter option for mild-to-moderate lateral ankle sprains and chronic instability. They wrap snugly around the ankle, compress soft tissue, and limit excessive inversion, which is the rolling motion that causes most sprains. Brands like Swede-O, ASO, and McDavid produce widely used lace-up models available at most sporting goods stores. These braces work well for athletes returning to sport after a Grade I or Grade II sprain.
Hinged and stirrup braces
Hinged or stirrup braces add rigid plastic shells on either side of the ankle, allowing up-and-down movement while blocking side-to-side motion. They are the preferred choice for moderate-to-severe sprains and early-stage rehabilitation after ligament injuries. The Aircast Air-Stirrup is one of the most clinically studied stirrup braces in podiatric practice. Patients with recurring instability often transition from a stirrup brace to a lace-up as strength and proprioception improve.
Walking boots (CAM boots)
Controlled ankle motion (CAM) boots, commonly called walking boots, are removable devices that encase the foot and lower leg in a rigid shell. Walking boots allow adjustable immobilization and controlled ankle movement, making them suitable for stable fractures, severe ligament tears, and post-surgical recovery. Unlike plaster casts, boots are removable for skin care and hygiene. That convenience matters for patients managing wounds or monitoring healing skin.
Custom ankle-foot orthoses (AFOs)
Custom AFOs are prescription devices fabricated from a scan or mold of your foot and lower leg. OTC braces do not adequately address complex neurological or severe structural conditions, which require prescription AFOs with tailored control. Conditions like foot drop, posterior tibial tendon dysfunction (PTTD), and Charcot neuroarthropathy require this level of customization. Stridefootankle provides general foot and ankle care that includes evaluation for custom AFO candidacy.
Brace type comparison
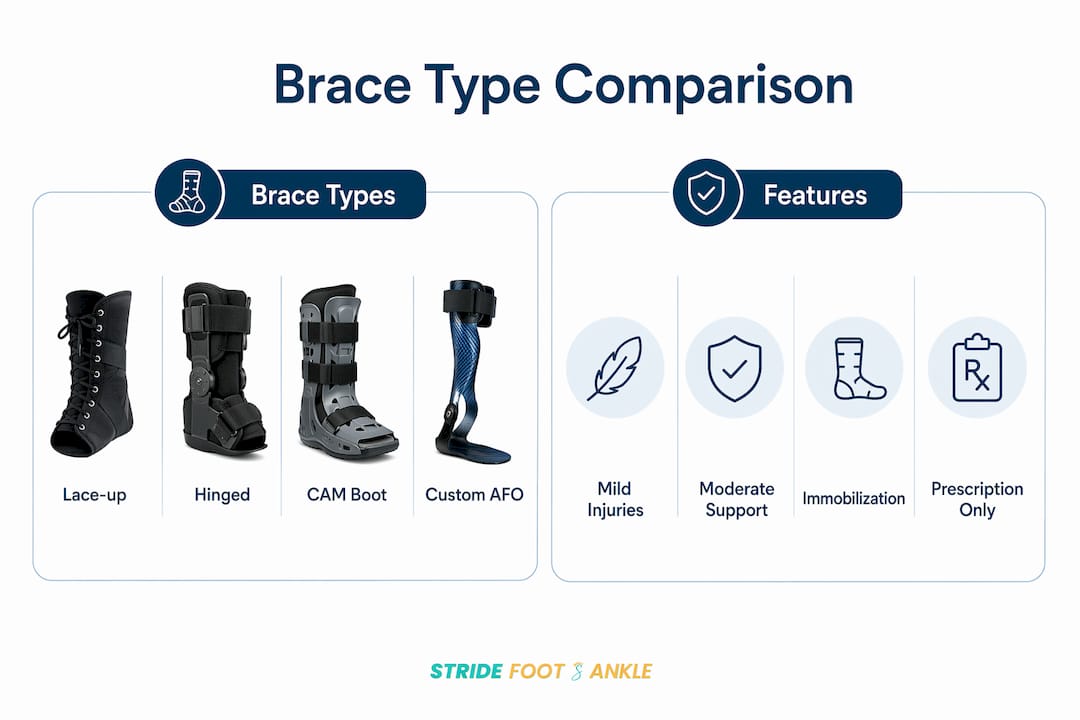
| Brace type | Best for | Mobility level | Prescription needed? |
|---|---|---|---|
| Lace-up ankle brace | Mild-to-moderate sprains, instability | High | No |
| Hinged/stirrup brace | Moderate-to-severe sprains, rehab | Moderate | No |
| CAM walking boot | Fractures, severe tears, post-surgery | Low | Usually yes |
| Custom AFO | Neurological conditions, PTTD, drop foot | Variable | Yes |
How does bracing prevent injuries and support recovery?
Bracing reduces the risk of both first-time and recurrent ankle injuries by limiting the mechanical range of motion that leads to sprains. Ankle bracing reduces first-time and recurrent ankle injuries significantly, with relative risk reductions of 0.53 for primary prevention and 0.37 for secondary prevention. That means a properly braced ankle is nearly two-thirds less likely to suffer a repeat sprain. For anyone with a history of ankle instability, that number alone makes bracing a non-negotiable part of returning to sport.
The benefits extend beyond the physical. Ankle bracing improves mechanical stability and provides psychological confidence that is critical for returning to activity after injury. Patients who feel supported move more naturally and are less likely to guard or compensate in ways that create secondary problems in the knee or hip.
Functional bracing also speeds recovery in specific injury types. Functional bracing enables a faster return to sport compared to casting in many severe ankle sprains. Casting locks the joint completely, which can cause muscle atrophy and stiffness. A well-fitted stirrup brace or CAM boot maintains enough stability to protect healing tissue while letting you walk and perform controlled exercises.
Key recovery benefits of ankle bracing include:
- Reduced reinjury risk through mechanical restriction of harmful motion
- Maintained muscle activation because the joint still moves within a safe range
- Faster return to weight-bearing compared to full immobilization in casts
- Improved proprioception feedback, helping the nervous system relearn balance
- Psychological reassurance that reduces fear-avoidance behavior during rehab
For patients managing tendon and ligament injuries without surgery, bracing is often the cornerstone of the entire treatment plan.
Pro Tip: If you play basketball, soccer, or volleyball, wear your ankle brace during every practice session, not just games. Most reinjuries happen during training when fatigue reduces neuromuscular control.
How to choose the right brace for your foot or ankle condition?
Choosing the correct brace starts with an accurate diagnosis. Self-diagnosis leads to mismatched devices that either under-protect a serious injury or over-restrict a minor one. A podiatrist or orthopedic specialist can identify the exact structure involved, the severity of damage, and the functional demands of your daily life before recommending a device.
Follow these steps to make an informed decision:
Get a professional diagnosis first. Pain at specific points, such as the base of the fifth metatarsal, requires imaging before any brace is applied. Wraps and OTC braces provide minimal stabilization and are insufficient for suspected fractures.
Match the device to the injury severity. Grade I sprains respond well to lace-up braces. Grade II and III sprains typically need a stirrup brace or CAM boot. Fractures and post-surgical cases require physician-prescribed immobilization.
Consider your activity goals. A recreational walker needs different support than a competitive runner. Performance trade-offs exist with bracing; braces reduce injury risk but may affect complex agility movements, so selection must be individualized.
Understand weight-bearing instructions. Wearing a boot does not automatically mean no weight-bearing; your physician must specify your weight-bearing status. Assuming you can walk in a boot without guidance is one of the most common and damaging mistakes patients make.
Ask about insurance and prescription requirements. Custom AFOs require a prescription and are often covered by insurance when medically necessary. OTC braces are not typically reimbursable. Stridefootankle can assist with documentation and insurance coordination for custom devices.
Avoid the “more is better” trap. Wearing a rigid brace for a mild sprain can weaken the surrounding muscles over time. The goal is the minimum restriction needed to protect the injury while allowing therapeutic movement.
Pro Tip: Bring your most-used footwear to your appointment. The fit between your brace and shoe matters as much as the brace itself. A brace that does not fit inside your shoe will not be worn consistently, and inconsistent use eliminates most of the protective benefit.
OTC braces address lateral instability from sprains, while custom AFOs control foot and ankle position for complex conditions like drop foot and arthritis. If your condition falls into the complex category, an OTC device will not deliver the control you need.
Tips for proper use, care, and integration of bracing in rehabilitation
A brace only works when worn correctly and consistently. Fit, hygiene, and integration with physical therapy all determine whether your device accelerates recovery or sits unused in a drawer.
Fitting and wearing your brace correctly
Put your brace on before you get out of bed in the morning if your physician recommends full-day wear. Swelling is lowest after rest, and fitting the brace at that point gives you the most accurate compression. Lace-up braces should feel snug but not cut off circulation. Check for numbness, tingling, or skin redness after the first hour of wear, and loosen the brace if any of these appear.
For CAM boots, follow your physician’s instructions on the number of air bladder pumps precisely. Over-inflating the boot creates pressure sores. Under-inflating reduces immobilization and defeats the purpose of the device.
Daily activity and sports use
Wear your brace for all weight-bearing activities during the prescribed period, including short walks to the kitchen. Many patients remove their brace for “just a quick trip” and re-injure themselves on that exact trip. For athletes cleared to return to sport, preventing ankle ligament reinjury requires consistent brace use through the full return-to-sport protocol, not just the first few sessions back.
Brace care and hygiene
- Wash lace-up fabric braces every two to three days in cold water with mild detergent. Air dry only. Machine drying warps the structure.
- Wipe plastic stirrup and CAM boot shells with an antibacterial wipe daily. Bacteria accumulate quickly in warm, enclosed environments.
- Inspect the lining of your boot or brace weekly for cracks, worn padding, or broken closures. A damaged brace provides unpredictable support.
- Replace OTC braces every three to six months with heavy daily use. Elastic and foam components lose their mechanical properties over time.
Combining bracing with physical therapy
Bracing should complement rehabilitation, not replace it. Physical therapy targeting peroneal muscle strength, calf flexibility, and single-leg balance is what builds the long-term stability that eventually lets you reduce or eliminate brace dependence. A brace worn without any strengthening program creates a cycle of dependency where the joint never fully recovers its natural stability.
Seek medical reassessment if you experience any of the following while braced:
- Increased pain or swelling after the first 48–72 hours of use
- Skin breakdown, blistering, or open sores under the device
- Numbness or tingling that persists after loosening the brace
- No functional improvement after two to four weeks of consistent use
Key takeaways
The most effective bracing outcome depends on matching the correct device to the specific injury, wearing it consistently, and combining it with active rehabilitation exercises.
| Point | Details |
|---|---|
| Match brace to injury severity | Lace-up braces suit mild sprains; CAM boots and AFOs address fractures and complex conditions. |
| Bracing cuts reinjury risk significantly | Functional ankle bracing reduces recurrent sprain risk by up to 63%, making it critical for active patients. |
| Boots do not equal non-weight-bearing | Always confirm weight-bearing status with your physician; a boot alone does not define your activity restrictions. |
| Combine bracing with physical therapy | Bracing without strengthening exercises creates dependency and delays full recovery of natural joint stability. |
| Replace and inspect devices regularly | OTC braces lose mechanical effectiveness within three to six months of heavy use and must be replaced. |
Why I think most patients underestimate what a brace actually does
Most people treat a brace like a bandage. They put it on, feel better, and assume the injury is handled. That mindset is where recovery stalls.
What a brace actually does is buy you time. It holds the joint in a protected position long enough for the tissue to repair itself and for your nervous system to relearn how to stabilize the ankle without thinking about it. The brace is not doing the healing. Your body is. The brace just keeps you from undoing that work every time you take a step.
The part that surprises most patients is the psychological dimension. Research confirms that bracing acts both physically and mentally to reduce reinjury risk. Patients who feel supported move more confidently. That confidence is not false. It translates into better movement patterns and fewer compensatory habits that create secondary injuries in the knee or hip.
Where I see patients go wrong most often is in two opposite directions. Some wear their brace far too long and never do the strengthening work that makes the brace unnecessary. Others ditch the brace too early because they feel fine, then re-injure themselves within weeks. The right path is a structured progression: brace for protection, therapy for strength, then a gradual reduction of brace dependence as the joint earns back its stability.
The other thing worth saying plainly: an OTC brace from a pharmacy is not a substitute for a diagnosis. If you are not sure what you injured, get imaging. A lace-up brace on an undiagnosed fracture is not treatment. It is a delay that makes the eventual treatment harder.
— Ramil
Get expert bracing guidance at Stridefootankle
Choosing the right brace without professional guidance is a gamble that often costs more time and pain in the long run. At Stridefootankle, Dr. Nahad Wassel evaluates your specific injury, activity level, and recovery goals to prescribe the device that fits your life, not just your diagnosis.

From conservative foot and ankle care to custom AFO fabrication and insurance documentation support, Stridefootankle provides the full spectrum of bracing services for Las Vegas patients. Whether you are dealing with a first-time sprain or managing a complex condition like PTTD or post-surgical recovery, the team at Stridefootankle can match you with the right device and the right rehabilitation plan. Schedule your consultation today and get back on your feet with confidence.
FAQ
What is the difference between an ankle brace and a walking boot?
An ankle brace provides functional support and limits harmful motion while allowing normal walking, making it suitable for mild-to-moderate sprains. A walking boot provides rigid immobilization for severe injuries, fractures, or post-surgical recovery, and your physician must specify whether weight-bearing is permitted while wearing it.
Can I buy an ankle brace without a prescription?
Most lace-up and hinged stirrup braces are available over the counter without a prescription. Custom AFOs require a physician’s prescription and are fabricated from a mold or scan of your foot; these are necessary for complex conditions like foot drop, PTTD, or severe arthritis.
How long should I wear a brace after an ankle sprain?
Wearing time depends on sprain severity. Grade I sprains typically require bracing for two to four weeks during activity. Grade II and III sprains may require six to twelve weeks of consistent use, combined with physical therapy, before brace dependence is safely reduced.
Does wearing a brace weaken my ankle over time?
A brace worn without accompanying strengthening exercises can reduce the muscle activation that builds long-term stability. The solution is to treat bracing as a temporary scaffold while you complete a physical therapy program targeting peroneal strength, calf flexibility, and balance, then gradually reduce brace use as your joint recovers.
When should I see a podiatrist instead of self-treating with a brace?
See a podiatrist if you have pain directly over a bone, significant swelling within the first hour of injury, inability to bear weight, or no improvement after 48–72 hours of bracing and rest. Pain at the base of the fifth metatarsal specifically requires imaging before any brace is applied, as this location is a common fracture site that OTC braces cannot adequately protect.
Recommended
- Previous Injury: Foot & Ankle Recovery Guide 2026 – Stride Foot & Ankle – Dr. Nahad Wassel
- Ankle Sprain Recovery Process: Your 2026 Rehab Guide – Stride Foot & Ankle – Dr. Nahad Wassel
- How to prevent foot injuries: expert strategies for healthy feet – Stride Foot & Ankle – Dr. Nahad Wassel
- Sports Injuries: Treatment, Prevention, and Recovery Guide – Stride Foot & Ankle – Dr. Nahad Wassel
Recent Comments