
TL;DR:
- Most pediatric foot variants, like flat feet and in-toeing, are normal developmental stages that resolve with time. Observation of symptoms, flexibility, and progress over months are more informative than immediate intervention; pain or rigidity warrant seeking professional evaluation. Trust your child’s natural growth, and consult experts when persistent symptoms or concerns arise.
As a parent in Las Vegas, watching your child take their first steps is one of the most exciting milestones you’ll ever witness. But it’s also when many parents start noticing things that look a little off: flat arches, feet that point inward, or a toddler who insists on walking on their tiptoes. The instinct to worry is completely natural. What’s surprising, though, is that the vast majority of these observations are entirely normal parts of childhood development, and with a little knowledge, you can tell the difference between what just needs time and what genuinely needs a closer look.
Table of Contents
- Understanding pediatric foot development: What’s normal?
- Common alignment variants and their progression
- Toe walking: When is it normal and when to seek help?
- Symptomatic conditions: When pain or persistent symptoms occur
- Our experience: What most articles miss about pediatric foot problems
- Connect with expert care in Las Vegas
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Most foot issues resolve | Flexible flat feet and alignment problems in early childhood usually improve naturally. |
| Watch for persistent symptoms | Pain, rigidity, or symptoms lasting beyond age 5-8 often require medical evaluation. |
| Toe walking mostly outgrown | Toe walking is common but persistent cases should be evaluated beyond age 5. |
| Parent observation is vital | Monitoring development and noting persistent or painful issues helps guide timely care. |
| Local specialty care available | Las Vegas families can access expert pediatric foot care for peace of mind and healthy development. |
Understanding pediatric foot development: What’s normal?
Children’s feet are not simply small versions of adult feet. They go through a remarkable series of changes from birth through adolescence, and the timeline varies widely from child to child. Understanding what’s happening at each stage can save you a lot of anxiety and help you make better decisions about when to call a specialist.
When babies are born, their feet are mostly made up of cartilage, which gradually hardens into bone over the first several years of life. This is why newborns and toddlers have that adorable chubby foot appearance, and why it’s completely normal for very young children to look flat-footed. The arch you expect to see simply hasn’t formed yet.
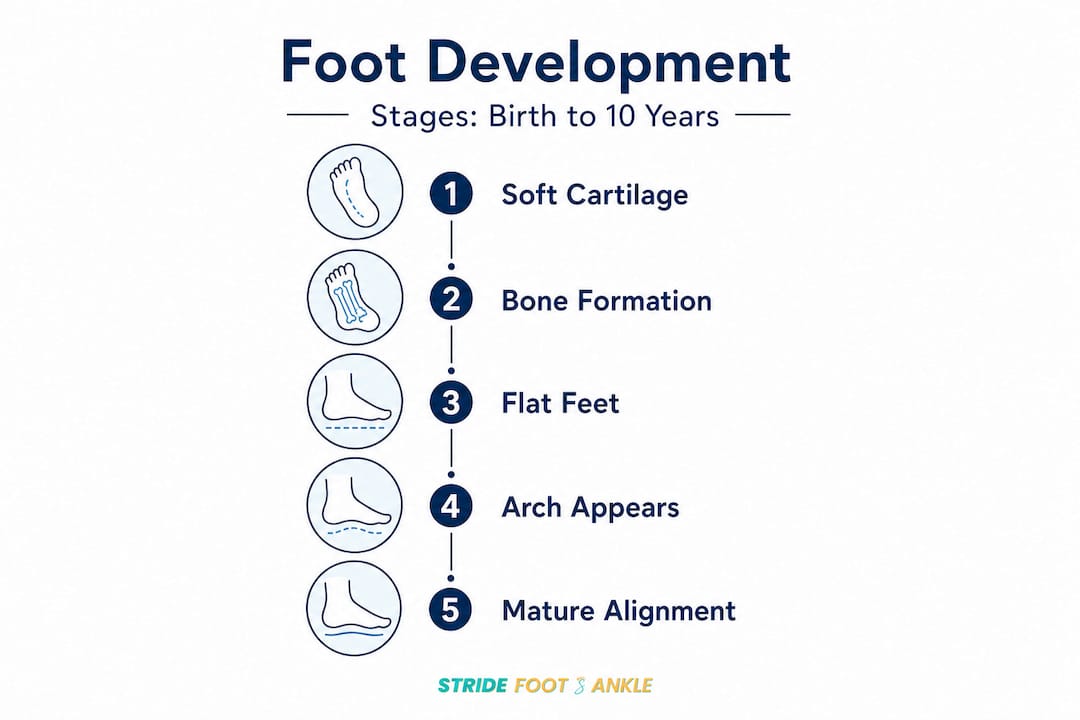
The mature medial arch typically develops between ages 6 and 10, and roughly two-thirds of children have painless, functional flexible flat feet throughout their early years. This means the arch disappears when the child stands and reappears when they go up on their tiptoes or sit with their feet off the floor. This is not a problem. It’s biology doing exactly what it should.
Similarly, leg and foot alignment issues that look alarming to parents are often predictable developmental phases. Conditions like bow legs, knock knees, in-toeing (feet pointing inward), and out-toeing (feet pointing outward) are extremely common in young children. The good news is that leg alignment problems like these often correct themselves with growth, with flat feet frequently resolving by around age 6 if an arch forms when the child stands on tiptoe.
Here’s a helpful comparison to guide your thinking:
| Condition | Typical age it appears | Typical age it resolves | When to be concerned |
|---|---|---|---|
| Flexible flat feet | Infancy to toddlerhood | 6 to 10 years | If painful, rigid, or still present after age 10 |
| Bow legs | Birth to 18 months | 2 to 3 years | If worsening, unequal, or severe past age 3 |
| Knock knees | 3 to 4 years | 6 to 7 years | If severe, worsening, or causing pain or limping |
| In-toeing | 1 to 3 years | By age 8 | If painful, one-sided only, or worsening over time |
| Out-toeing | Early toddlerhood | 3 to 4 years | If persistent past age 5 or associated with hip issues |
The key distinction is between flexible and rigid presentations. A flexible flat foot corrects when the child rises on tiptoe. A rigid flat foot stays flat no matter what position the foot is in, and that’s the kind that warrants further evaluation. The same logic applies to other alignment variants: flexibility and painlessness are reassuring, while rigidity and pain are red flags.
For general foot and ankle care, the first step is always observation. Watching how your child walks, runs, and plays over weeks and months gives you and your doctor far more useful information than a single snapshot in time.
Key takeaway: Most pediatric foot and leg alignment variants are normal developmental stages. Observation is your first and most powerful tool. Pain, rigidity, and persistence beyond expected ages are the clearest signals that something needs clinical attention.
Here are some reassuring signs that your child’s feet are developing normally:
- The arch appears when your child stands on tiptoe or sits with feet hanging
- Your child walks, runs, and plays without pain or complaint
- Both feet look and function similarly
- The condition has been improving gradually as your child grows
- Your child’s balance and coordination are age-appropriate
Common alignment variants and their progression
Now that you’ve seen the big picture of normal development, let’s break down specific alignment issues and how they typically change as your child grows.
In-toeing, where the toes point inward during walking, is one of the most frequently mentioned concerns in pediatric foot care. It has three main causes depending on the child’s age: metatarsus adductus (a curved forefoot, usually from positioning in the womb), internal tibial torsion (a twist in the shinbone), and femoral anteversion (a rotation in the thighbone). Most cases of in-toeing resolve without treatment by age 8, and corrective shoes or braces are generally not recommended because research hasn’t shown they speed up resolution.

Out-toeing is when the feet point outward during walking. It’s less common than in-toeing but follows a similar pattern of self-correction in most children. If it persists or is combined with tripping, pain, or significant imbalance, it’s worth discussing with a specialist.
Bow legs (genu varum) are normal from birth through about 18 months. After that, they typically straighten as the child begins bearing full weight and walking. If bow legs are still pronounced after age 3, are getting worse rather than better, or are clearly more severe on one side, further evaluation is needed to rule out conditions like Blount’s disease or rickets.
Knock knees (genu valgum) appear later, usually around ages 3 to 4, when bow legs naturally overcorrect during development. Most children’s knees straighten out by age 6 or 7. Severe or worsening knock knees, or those that are causing a child to trip frequently or experience knee pain, are worth evaluating.
Understanding that these conditions follow a natural arc of development helps you set appropriate expectations. Here’s what to watch for over time:
- Is the condition improving, staying the same, or getting worse?
- Is your child in pain, limping, or avoiding physical activity?
- Does the condition affect one side significantly more than the other?
- Is your child reaching other motor milestones at the expected pace?
Pro Tip: Take short video clips of your child walking on a flat surface every few months. This gives you a visual record that is far more useful during a clinical appointment than trying to remember what you observed weeks ago.
Being proactive about preventing foot injuries in children also includes choosing appropriate footwear. Shoes should fit well, provide adequate support, and allow room for the toes to move. Stiff shoes, shoes that are too small, or shoes that are handed down and molded to another child’s foot shape can all affect how your child’s feet develop. Barefoot time on safe surfaces is actually healthy for young children because it builds foot strength and sensory awareness.
Toe walking: When is it normal and when to seek help?
Toe walking, where a child walks on the balls of their feet with heels off the ground, is something many parents notice and worry about. The reality is more nuanced than most expect.
In toddlers between the ages of 1 and 3, toe walking is often completely normal. Children at this age are still figuring out how their bodies work, and toe walking is frequently just a phase of motor exploration. Many children toe walk some of the time and walk normally at other times, which is a very reassuring sign.
However, the picture changes if the behavior persists. Persistent toe walking beyond age 5 is not considered typical unless other medical conditions have been ruled out. After age 5, a child’s gait pattern is generally more established, and continued toe walking warrants a closer look.
Here’s a step-by-step guide to how toe walking is typically evaluated and managed:
- Observe the pattern. Does your child toe walk all the time or only sometimes? Can they bring their heels down when you ask them to? Occasional toe walking with the ability to walk flat-footed on request is much less concerning.
- Check for tight calf muscles. One of the most common physical findings in children who toe walk is reduced flexibility in the calf muscles and Achilles tendon. A simple test is to gently flex the foot upward (dorsiflex) while the knee is straight: there should be at least 10 to 15 degrees of motion.
- Start with stretching. Daily calf stretches are often the first-line recommendation for children with idiopathic (no known cause) toe walking. These stretches help maintain and improve ankle range of motion.
- Consider appropriate footwear. Shoes with a slight heel can sometimes make it easier for toe walkers to maintain heel contact, while minimalist shoes may not provide enough support for children with significant tightness.
- Seek evaluation if it persists past age 5. The SickKids-based guidance recommends seeing a healthcare provider if toe walking does not resolve by age 5, because neurological and musculoskeletal causes need to be ruled out before labeling it idiopathic.
Possible underlying causes that a clinician will consider include cerebral palsy, autism spectrum disorder, muscular dystrophies, and tight Achilles tendons that prevent normal heel-to-toe gait. This doesn’t mean every toe walker has a serious condition. It means a thorough evaluation helps you get clarity and put together the right plan.
Important reminder: Toe walking that is associated with developmental delays, speech delays, sensory sensitivities, or social communication differences may point toward autism spectrum disorder and deserves a multidisciplinary evaluation, not just a foot assessment.
Conservative foot care approaches for toe walking often include physical therapy to address muscle tightness and motor patterns. In some cases, custom orthotics or ankle-foot orthoses (AFOs, which are specialized braces) may be recommended. Serial casting, a process where casts are applied and changed every few weeks to gradually stretch the calf, is another option for children with significant Achilles tightness.
Pro Tip: If your child’s toe walking has been dismissed as “just a phase” but they are past age 5 and you still have concerns, trust your instincts and request a formal evaluation. A second opinion from a physical therapy specialist can provide real clarity and a structured treatment plan.
Symptomatic conditions: When pain or persistent symptoms occur
While most of what we’ve discussed so far falls under the category of normal developmental variants, there are genuine foot conditions in children that cause pain, disrupt activity, or indicate something that needs treatment. Recognizing the difference between a variant and a symptomatic condition is one of the most valuable things you can do as a parent.
It’s important to separate developmental variants like flexible flat feet, in-toeing, and transient toe walking from symptomatic conditions such as pain with activity like Sever’s disease, or skin conditions like rashes and blisters. These two categories require completely different responses.
Sever’s disease (calcaneal apophysitis) is the most common cause of heel pain in active children, typically between the ages of 8 and 14. It’s not actually a disease in the traditional sense. It’s an overuse injury that affects the growth plate in the heel. During growth spurts, the heel bone grows faster than the Achilles tendon, creating tension and inflammation at the growth plate. It’s especially common in Las Vegas children who are active in sports year-round due to the area’s warm climate.
Signs of Sever’s disease include:
- Heel pain that worsens with activity, especially running and jumping
- Pain at the back or bottom of the heel when squeezed from both sides
- Limping or walking on tiptoes to avoid heel contact
- Stiffness in the morning or after rest
- Pain that eases with rest but returns with physical activity
Plantar fasciitis is less common in children than in adults but does occur, particularly in older adolescents and in children who are flat-footed or very physically active. It presents as pain on the bottom of the heel, especially with the first steps in the morning.
Skin conditions on the feet are also worth knowing about. Foot fungus (athlete’s foot) causes itching, scaling, and redness between the toes and on the soles. It’s common in children who use community pools, locker rooms, and sports facilities. Plantar warts caused by the human papillomavirus (HPV) can appear on the soles of the feet and may be mistaken for calluses. They can be painful when pressed and often have small black dots (tiny clotted blood vessels) at their center.
Evidence-based guidance emphasizes that management often starts with observation and targeted exercises or shoe support, with further evaluation recommended when features are rigid, painful, progressive, or persistent beyond expected age ranges.
Signs that a symptomatic foot condition needs professional care include:
- Pain that limits your child’s participation in activities they normally enjoy
- Swelling, redness, or warmth in the foot or ankle
- Skin changes that don’t resolve on their own within a week or two
- A lump or bump on the foot that is tender or growing
- A child who is consistently limping or favoring one side
- Any foot concern in a child with diabetes, a neuromuscular condition, or other complex medical history
Our experience: What most articles miss about pediatric foot problems
Here’s something we see consistently in clinical practice that most general articles on this topic fail to address: parents often seek intervention far too early, and this can sometimes do more harm than good.
The overwhelming majority of children who come through our doors with flat feet, in-toeing, or toe walking turn out to be completely fine. Their feet just need time. But the well-meaning rush to “fix” something that isn’t broken can lead to unnecessary expenses, anxiety, and in some cases, ill-fitting orthotics or interventions that the evidence doesn’t support.
What clinical experience teaches you over time is that context matters enormously. A 3-year-old with flat feet is almost certainly developing normally. A 12-year-old with painful, rigid flat feet who is avoiding gym class is a different story entirely. The problem is that both situations might look similar in a photograph, but they are worlds apart clinically.
Patience and structured observation are genuinely underutilized tools in pediatric foot care. We encourage parents to document changes, track whether their child is in pain, and note whether the condition seems to be resolving over months rather than days. This kind of observational discipline gives everyone, parents and clinicians alike, much better information to work with.
The other thing most articles miss is that footwear choices during development genuinely matter, but not always in the direction parents expect. Heavily structured “supportive” shoes might actually slow the development of intrinsic foot muscle strength in young children. For toddlers learning to walk, flexible, well-fitting shoes or even safe barefoot time is often more beneficial than rigid orthopedic footwear.
When we do recommend intervention, it’s because symptoms are present, the condition is progressing, or there’s a meaningful impact on the child’s quality of life and activity level. Nonsurgical options for tendon and ligament issues are almost always the first path, and the results with appropriate conservative care are genuinely excellent in the pediatric population.
The honest truth is this: if your child is active, happy, and not in pain, they are almost certainly fine. Your worry is valid, but so is the reassurance that nature handles most of this beautifully on its own.
Connect with expert care in Las Vegas
Even when you know the facts, watching your child walk differently or hearing them complain about foot pain can be genuinely unsettling. You don’t have to figure it out alone.

At Stride Foot & Ankle, Dr. Nahad Wassel and our team offer expert, evidence-based pediatric foot care right here in Las Vegas. We understand the specific concerns of local families and approach every evaluation with the goal of giving you real answers, not unnecessary interventions. Whether your child needs a reassuring check-in or a structured treatment plan, our conservative foot care options are designed to support healthy foot development at every stage. From flexible flat feet and toe walking to Sever’s disease and skin conditions, we provide personalized guidance backed by current clinical evidence. Explore our full range of general foot and ankle care services or request an appointment today so your child can keep striding confidently forward.
Frequently asked questions
What age should the arch in my child’s foot become visible?
The foot arch typically develops and becomes visible between ages 6 and 10, with about two-thirds of young children having painless flexible flat feet before that stage.
Is it normal for children to walk on their toes?
Toe walking is common in toddlers and often resolves on its own, but it may require evaluation if it persists past age 5, as other medical conditions should be ruled out at that point.
When should I worry about my child’s flat feet?
Flat feet are usually normal in young children and often correct by age 6 if an arch forms when they stand on tiptoe; evaluation is recommended if the flat foot is painful, rigid, or persists well past age 10.
What signs indicate a pediatric foot issue needs medical attention?
Pain, rigidity, limping, or a condition that is worsening rather than improving are clear signs that a clinical evaluation is the right next step, especially when these features appear beyond the typical age range for self-correction.
Recommended
- How to prevent foot injuries: expert strategies for healthy feet – Stride Foot & Ankle – Dr. Nahad Wassel
- General Foot & Ankle Care – Stride Foot & Ankle
- How Conservative Foot Care Relieves Pain and Prevents Surgery – Stride Foot & Ankle – Dr. Nahad Wassel
- How to prepare for foot surgery: steps, recovery, and expert tips – Stride Foot & Ankle – Dr. Nahad Wassel
Recent Comments